INHBE siRNA
- Pre-clinical studies demonstrate fat-selective weight loss and off-treatment weight maintenance.
- Additional key IND-enabling study readouts in Q4 2025.
- Phase 1 FPI in Q1 2026.
Key Data
Based on in vitro and in vivo studies, VIAL-INHBE effectively demonstrates functional potency and target-binding comparable to or better than clinical programs.
- Vial's INHBE siRNA treatment leads to fat-selective weight loss and weight loss is maintained post-treatment cessation.
- Vial's INHBE siRNA supports fat loss maintenance post-GLP-1 treatment cessation.
- Vial's INHBE siRNA is synergistic with GLP-1 treatment to support added fat loss and weight loss.
- Lead series shows high stability in NHP liver lysates (S9 fractions) during the 72 hr incubation, indicating potential for a favorable dosing interval.
- Lead series displays robust knockdown potency in primary human hepatocytes, indicating potential for strong efficacy.
- Lead series displays low risk of immunogenicity in human PBMCs, indicating potential for a strong safety profile.
Differentiated Product Profile
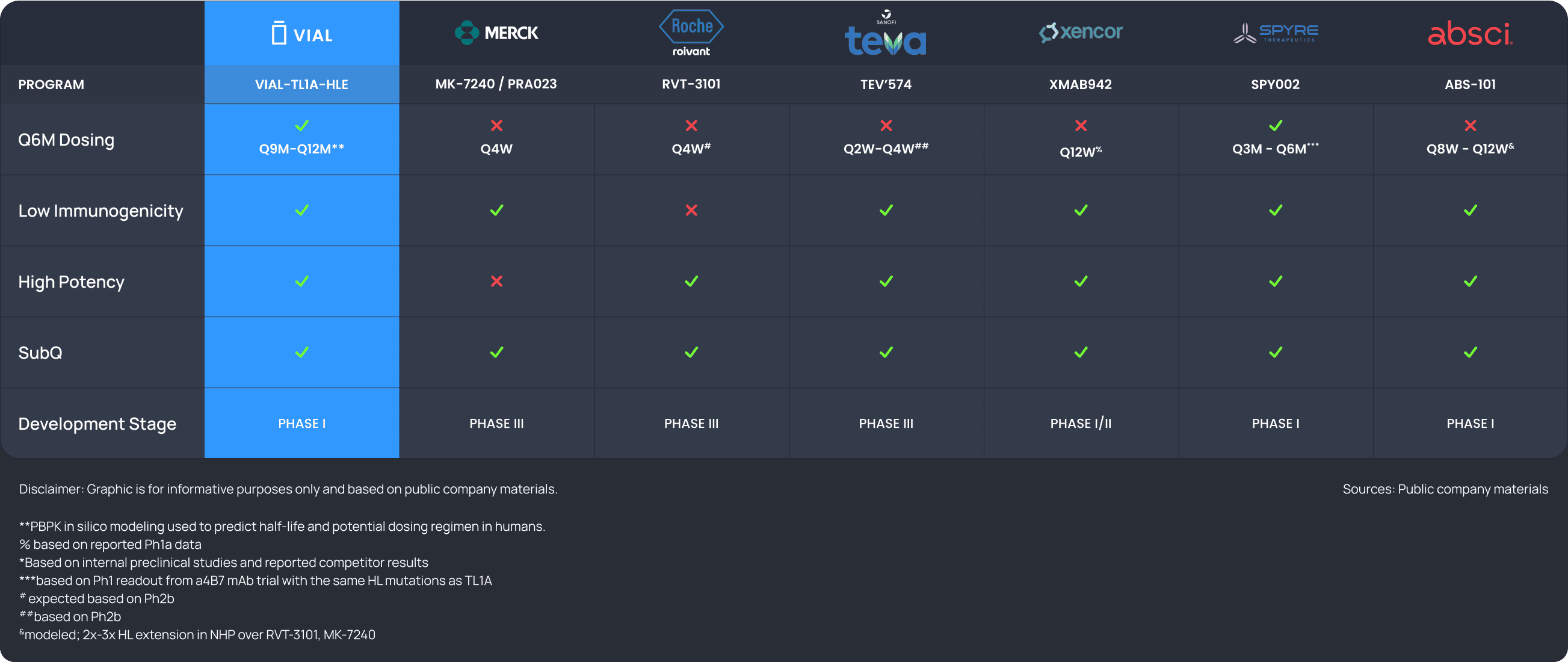
VIAL-TL1A-HLE is potentially a best-in-class anti-TL1A mAb with an extended half-life to support Q9-12M dosing, powered by Vial’s HLE platform. The program is also applicable to MASH, Atopic Dermatitis, SSc-ILD, Rheumatoid Arthritis, Hidradenitis Suppurativa, among others.
Updates
So 1st of all, TL1A Is one of the hot targets at the moment for both Crohn's and Uc. And one of the major challenges that we have in the clinic is to have drugs that need frequent administration and patients like to have drugs that are very effective and that are super safe, and that are easy to administer.
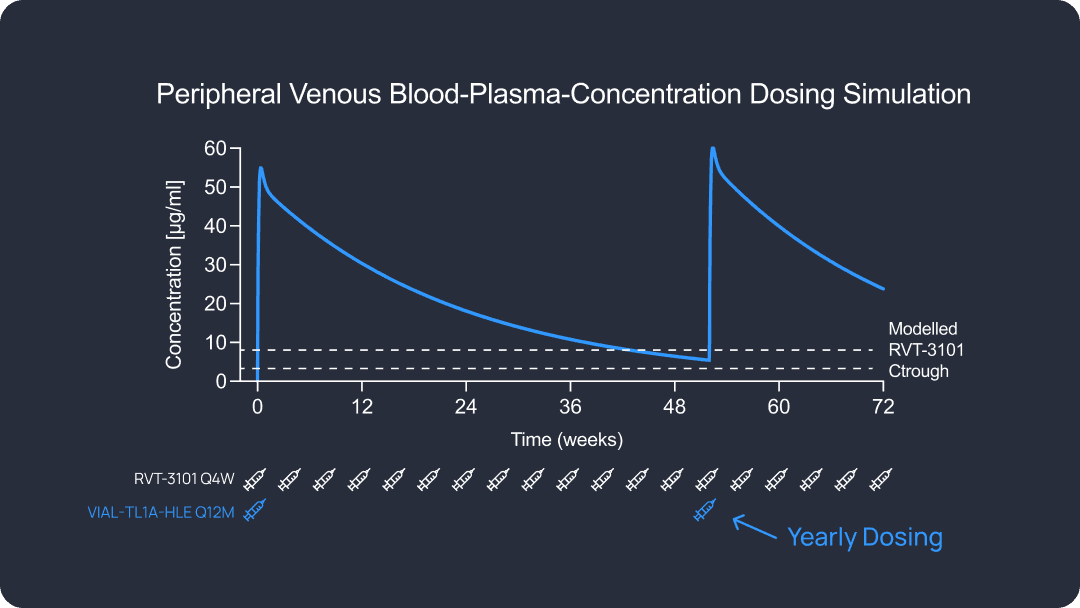
So instead of every 2 weeks, every month, having an injection every 6 months, or once a year, with a very safe mechanism of action. I mean, this is the ideal thing to have for a patient perspective and also for a doctor.
A long half-life reduces the burden on the patient hopefully provides a very steady state concentration of drug and binding of the target over the extended half-life, which in theory should be very good at preventing episodic flares.
I mean, IBD is a lifelong condition that requires long-term management. Many patients struggle with treatment, fatigue, adherence, challenges, and disruptions in daily life. So an extended half-life TL1A therapeutic, especially one with the potential for once yearly dosing, could significantly improve the quality of life, of reducing injection burden, minimizing clinic visits and maintaining consistent disease control.